Printable North Dakota Ems Patient Care Report Template
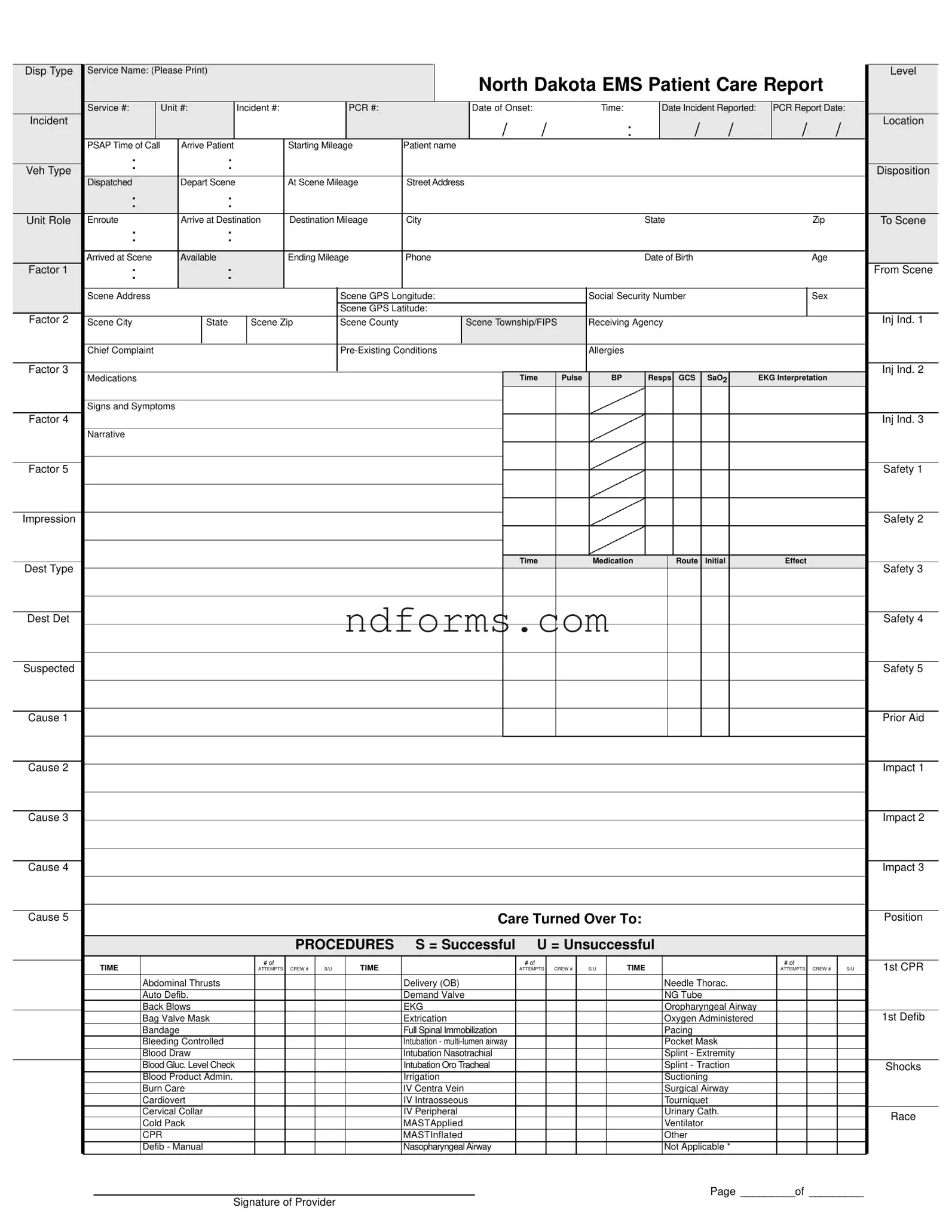
The North Dakota EMS Patient Care Report form encompasses a comprehensive framework designed for documenting the critical aspects of patient care administered by emergency medical services. This includes a gamut of information from basic identification details, such as the patient's name, age, and social security number, to more specific data related to the emergency incident—for instance, the location, time, and nature of the incident. Additionally, the form delves into the medical response details, capturing elements like initial assessments, administered medications, procedures attempted (noting successes or failures), and the patient’s vital signs over time. It also accommodates details regarding patient disposition, such as the type of receiving facility and patient mileage covered. Beyond the procedural and clinical information, the form ensures that the legal aspects, like consent or refusal of service, are clearly recorded, complemented by insurance and billing information to streamline the financial components of emergency medical care. Importantly, the form provides a structure for EMS providers to include narrative sections, allowing for a more detailed account of the patient's condition and the care provided. This fosters a holistic approach to patient care reporting, ensuring that every facet of the encounter is meticulously documented for legal, medical, and billing purposes.
Form Preview
Disp Type |
Service Name: (Please Print) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Level |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
North Dakota EMS Patient Care Report |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Service #: |
|
Unit #: |
Incident #: |
|
|
|
PCR #: |
|
|
|
Date of Onset: |
|
|
Time: |
|
|
Date Incident Reported: |
|
PCR Report Date: |
|
||||||||||||||||||
Incident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
|
|
: |
|
/ |
|
/ |
|
/ |
|
/ |
Location |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
PSAP Time of Call |
|
Arrive Patient |
|
|
|
Starting Mileage |
Patient name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Veh Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Disposition |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Dispatched |
|
Depart Scene |
|
|
|
At Scene Mileage |
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unit Role |
Enroute |
|
Arrive at Destination |
Destination Mileage |
City |
|
|
|
|
|
|
|
State |
|
|
|
|
|
Zip |
|
|
To Scene |
|||||||||||||||||
|
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Arrived at Scene |
|
Available |
|
|
|
Ending Mileage |
Phone |
|
|
|
|
|
|
|
Date of Birth |
|
|
|
|
|
Age |
|
|
|
||||||||||||||
Factor 1 |
: |
|
|
|
: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From Scene |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scene Address |
|
|
|
|
|
|
|
|
Scene GPS Longitude: |
|
|
|
|
Social Security Number |
|
|
|
|
|
Sex |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Scene GPS Latitude: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Factor 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 1 |
Scene City |
|
|
State |
|
Scene Zip |
|
Scene County |
|
|
Scene Township/FIPS |
Receiving Agency |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chief Complaint |
|
|
|
|
|
|
|
|
|
|
|
|
Allergies |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Factor 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 2 |
|
Medications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
Pulse |
|
BP |
|
Resps |
GCS |
|
SaO2 |
|
EKG Interpretation |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signs and Symptoms |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Factor 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inj Ind. 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Narrative |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Factor 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impression |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
|
|
Medication |
|
|
|
Route |
|
Initial |
|
|
|
Effect |
|
|
|
||||
Dest Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 3 |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dest Det |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suspected |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Safety 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Prior Aid |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Impact 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cause 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Care Turned Over To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Position |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROCEDURES |
S = Successful |
U = Unsuccessful |
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
# of |
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
TIME |
|
|
|
|
|
|
|
|
|
|
1st CPR |
|||||
|
|
|
|
|
|
|
|
ATTEMPTS |
CREW # |
S/U |
|
|
|
|
|
|
ATTEMPTS |
|
CREW # |
|
S/U |
|
|
|
|
|
|
|
|
ATTEMPTS |
CREW # |
|
S/U |
||||||
|
|
Abdominal Thrusts |
|
|
|
|
|
|
|
Delivery (OB) |
|
|
|
|
|
|
|
|
|
Needle Thorac. |
|
|
|
|
|
|
|
||||||||||||
|
|
Auto Defib. |
|
|
|
|
|
|
|
Demand Valve |
|
|
|
|
|
|
|
|
|
NG Tube |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Back Blows |
|
|
|
|
|
|
|
EKG |
|
|
|
|
|
|
|
|
|
Oropharyngeal Airway |
|
|
|
|
|
|
|
||||||||||||
|
|
Bag Valve Mask |
|
|
|
|
|
|
|
Extrication |
|
|
|
|
|
|
|
|
|
Oxygen Administered |
|
|
|
|
|
|
1st Defib |
||||||||||||
|
|
Bandage |
|
|
|
|
|
|
|
Full Spinal Immobilization |
|
|
|
|
|
|
|
|
|
Pacing |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Bleeding Controlled |
|
|
|
|
|
|
|
Intubation - |
|
|
|
|
|
|
|
|
|
Pocket Mask |
|
|
|
|
|
|
|
||||||||||||
|
|
Blood Draw |
|
|
|
|
|
|
|
Intubation Nasotrachial |
|
|
|
|
|
|
|
|
|
Splint - Extremity |
|
|
|
|
|
|
|
||||||||||||
|
|
Blood Gluc. Level Check |
|
|
|
|
|
|
|
Intubation Oro Tracheal |
|
|
|
|
|
|
|
|
|
Splint - Traction |
|
|
|
|
|
|
Shocks |
||||||||||||
|
|
Blood Product Admin. |
|
|
|
|
|
|
|
Irrigation |
|
|
|
|
|
|
|
|
|
Suctioning |
|
|
|
|
|
|
|
||||||||||||
|
|
Burn Care |
|
|
|
|
|
|
|
IV Centra Vein |
|
|
|
|
|
|
|
|
|
Surgical Airway |
|
|
|
|
|
|
|
||||||||||||
|
|
Cardiovert |
|
|
|
|
|
|
|
IV Intraosseous |
|
|
|
|
|
|
|
|
|
Tourniquet |
|
|
|
|
|
|
|
||||||||||||
|
|
Cervical Collar |
|
|
|
|
|
|
|
IV Peripheral |
|
|
|
|
|
|
|
|
|
Urinary Cath. |
|
|
|
|
|
|
Race |
||||||||||||
|
|
Cold Pack |
|
|
|
|
|
|
|
MASTApplied |
|
|
|
|
|
|
|
|
|
Ventilator |
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
CPR |
|
|
|
|
|
|
|
MASTInflated |
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Defib - Manual |
|
|
|
|
|
|
|
Nasopharyngeal Airway |
|
|
|
|
|
|
|
|
|
Not Applicable * |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page _________of _________
Signature of Provider
Patient Name (PLEASE PRINT)
North Dakota EMS Patient Care Report
|
|
|
BILLING INFORMATION |
|
|
|
|
|
|
MILEAGE |
|
INSURANCE TYPE |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance - Primary |
Number: |
Insurance - Secondary |
Number: |
|
Beg: |
|
|
|
❏ No Insurance |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Private Pay |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Responsible Party: |
|
|
|
|
|
|
|
End: |
|
|
|
❏ Private Insurance |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Medicare |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Last Name) |
|
(First Name) |
|
|
|
(MI) |
|
Total: |
|
|
|
❏ Medicaid |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Medicare/Medicaid |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Address) |
|
|
|
|
|
|
|
|
|
|
|
❏ VA Insurance |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(City) |
(State) |
(Zip) |
|
|
(Phone) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ Not Applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECEIPT OF SERVICE |
|
|
|
|
|
|
REFUSAL OF SERVICE |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
I acknowledge receipt of the EMS services listed in this document and accept |
This is to certify that I am refusing treatment / transport. I have been informed |
|||||||||||||
|
full responsibility for all charges. I authorize payment of medical benefits from |
of the risk(s) involved, and hereby release the ambulance service, its atten- |
|||||||||||||
|
my insurance company to provide of such services and authorize the provider |
dants, and its affiliates, from all responsibility which may result from this action. |
|||||||||||||
|
to release medical and other necessary information to my insurance company |
|
|
|
|
|
|
|
|
|
|||||
|
for that purpose. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Patient Signature |
|
|
Date/Time |
Patient Signature |
|
|
|
Date/Time |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CREW |
|
CREW MEMBER NAMES |
|
|
|
|
STAFF ID |
|
DRIVER |
LEVEL |
||||
1 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EKG STRIPS
File Attributes
| Fact Name | Fact Description |
|---|---|
| Form Use | Used by EMS providers to document care given to patients. |
| Governing Law(s) | The form is governed by North Dakota state EMS regulations and guidelines. |
| Information on Provider | Includes service name, service level, and crew member information. |
| Incident Details | Captures information such as incident number, location, time, and type of call. |
| Patient Information | Collects patient's name, date of birth, age, social security number, and medical information including pre-existing conditions and allergies. |
| Treatment and Procedures | Details treatments given, medications administered, procedures performed, and their outcomes. |
| Transportation Details | Records vehicle type, destination, and mileage related to the patient's transportation. |
| Billing Information | Includes insurance details, responsible party, and acknowledgment of service receipt or refusal. |
How to Write North Dakota Ems Patient Care Report
Filling out the North Dakota EMS Patient Care Report form is an important step in documenting the medical care provided during an emergency. This process ensures that patient care is thoroughly recorded for legal, medical, and insurance purposes. Here is a step-by-step guide on how to accurately complete the form.
- Start by entering the Disp Type, Service Name, and Level at the top of the form. Make sure to print legibly.
- Fill in the Service #, Unit #, Incident #, and PCR # to accurately identify the report.
- Record the Date of Onset, Time, Date Incident Reported, and PCR Report Date to log when the incident occurred and when it was reported.
- Under Incident Location, enter the PSAP Time of Call, Arrive Patient, Starting Mileage, Street Address, City, State, and Zip to outline where the incident took place and the response details.
- Detail the Veh Type, Disposition, Dispatched, Depart Scene, At Scene Mileage, Unit Role Enroute, Arrive at Destination, and Destination Mileage for complete vehicle and dispatch information.
- Provide the Patient's name, Date of Birth, Age, Phone, and Insurance Information including primary and secondary numbers, if applicable. Ensure to document the Responsible Party's information for billing purposes.
- Under the scene information, fill in the Scene Address, Scene GPS Longitude and Latitude, Social Security Number, Sex, and the Scene City, State, Zip, County, Township/FIPS.
- List any Receiving Agency, Chief Complaint, Pre-Existing Conditions, Allergies, Medications, and Impression to provide a comprehensive medical report.
- Document the Factor 1-5, Inj Ind., Time, Pulse, BP, Resps, GCS, SaO2, EKG Interpretation, and Signs and Symptoms for a detailed account of the patient's condition and the care provided.
- Complete the Narrative section with a detailed account of the incident, the care provided, and any observations relevant to the patient's condition.
- In the Procedures section, indicate any medical procedures performed by marking the appropriate boxes and providing details such as Time, # of Attempts, Crew #, and whether each was S (Successful) or U (Unsuccessful).
- For billing, fill in the Mileage, Insurance Type, and circle the relevant options concerning the insurance and payment responsibilities.
- Ensure Receipt of Service or Refusal of Service is signed by the patient or a representative to acknowledge the receipt or refusal of EMS services provided.
- Document the Crew Member Names, Staff ID, and indicate the Driver Level for each crew member involved in the service.
- Finally, make sure to sign the form in the Signature of Provider section, enter the page number, and provide the Patient's Name to authenticate the report.
After completing the North Dakota EMS Patient Care Report form, it's essential to review the document for accuracy and completeness. Once finalized, submit the form as directed by your EMS agency's protocol. This careful documentation ensures that the patient's care is accurately recorded for all parties involved, maintaining a high standard of medical accountability and service.
Your Questions, Answered
-
What is the North Dakota EMS Patient Care Report form?
The North Dakota EMS Patient Care Report form is a comprehensive document used by emergency medical services (EMS) to record all aspects of patient care during an EMS incident. This includes information about the call, patient data, clinical interventions, medications administered, and the outcome of the emergency response.
-
Who needs to fill out the North Dakota EMS Patient Care Report form?
EMS personnel who attend to patients during emergency calls are responsible for completing the form. This includes paramedics, emergency medical technicians (EMTs), and any other EMS providers who directly contribute to patient care.
-
What information is required in the Service Name and Level section?
In the Service Name and Level section, the EMS staff should clearly print the name of the EMS service provider and indicate the level of service provided, such as basic life support (BLS), advanced life support (ALS), or other specified levels of care.
-
How should incident-related times be recorded on the form?
Incident-related times including the time of the initial call, time dispatched, time arrived at the scene, and time left the scene should be accurately recorded. This helps in understanding the timeline of the EMS response and patient care process.
-
What details are required in the Patient Information section?
The Patient Information section requires detailed information about the patient, including their name, address, date of birth, age, sex, social security number (optional), and any relevant medical history like allergies or pre-existing conditions.
-
How is the Medical Intervention section utilized?
In the Medical Intervention section, EMS personnel document any procedures performed, medications administered, and the patient's response to treatment. Specific details such as the time of intervention, medication dosage, and the outcome of each procedure are recorded.
-
What is the purpose of the Billing Information section?
The Billing Information section captures data necessary for the EMS provider to bill for services rendered. This includes insurance information, mileage covered during the service, and the type of insurance coverage the patient has.
-
How is the Refusal of Service documented?
If a patient refuses EMS services or transportation, this decision is documented in the Refusal of Service section. The patient's signature is required to confirm that they understand the risks of refusing service and to release the EMS personnel from liability related to this decision.
-
What happens if there are multiple pages to the report?
Should the EMS Patient Care Report extend beyond one page, each additional page must be appropriately numbered. The provider's signature and the patient's name are required on each page to ensure continuity and proper documentation across the entire report.
-
Can EMS personnel add narrative descriptions to the report?
Yes, the Narrative section is designed for EMS personnel to provide a detailed description of the incident, the care provided, patient responses, and any other relevant observations not covered in the standard fields of the form.
Common mistakes
When filling out the North Dakota EMS Patient Care Report form, it is crucial to provide accurate and complete information. However, mistakes can happen. Here are seven common errors that individuals might make on the form:
- Leaving the Service Name or Service Number sections blank. These fields are essential for identifying the EMS service provider involved.
- Incorrectly reporting the Date of Onset and Time, alongside the Date Incident Reported and PCR Report Date. Accurate reporting of these dates and times is crucial for record-keeping and potentially for legal reasons.
- Not providing complete Location details, including the Street Address, City, State, Zip, and Scene GPS Coordinates. This information is critical for documenting where the incident occurred accurately.
- Failing to fill in the Patient Name, Date of Birth, Age, Sex, and Social Security Number correctly. This personal information is required for patient identification and billing purposes.
- Omitting or inaccurately listing Chief Complaint, Pre-Existing Conditions, Allergies, and Medications. This medical information is vital for providing appropriate care and for medical records.
- Skipping the Procedures section, including Time, Procedure Performed, and whether it was Successful (S) or Unsuccessful (U). This section is essential for documenting the care provided during the incident.
- Forgetting to include billing information, such as Insurance Type, Insurance Number, and Responsible Party. Accurate billing information is necessary for processing payment for the services rendered.
It is advisable to review the form carefully before submission to ensure all required information is accurately and fully provided. This attention to detail can help avoid unnecessary delays in patient care reporting and billing processes. Additionally, clear and complete documentation in the North Dakota EMS Patient Care Report form is essential for maintaining accurate medical records and facilitating quality patient care.
- Ensure all sections of the form are filled out, leaving no relevant fields blank.
- Double-check that all dates, times, and numerical information are entered correctly.
- Review the patient's information for accuracy, including personal and medical details.
- Confirm that the procedures performed are documented thoroughly, along with their outcomes.
- Verify that insurance and billing information is complete and accurate to facilitate proper billing.
By avoiding these common mistakes, individuals can help ensure that the patient care report is a useful and accurate document that supports high-quality care and efficient administrative processes.
Documents used along the form
The North Dakota EMS Patient Care Report form is crucial for documenting patient care during emergency medical services (EMS) operations. However, to complete a thorough documentation and billing process, other forms and documents are often needed alongside it. These additional forms ensure comprehensive patient care records, facilitate proper billing, and comply with legal and health regulations.
- Consent for Treatment Form: This document is vital, as it records the patient's consent to receive medical treatment. It's crucial in situations where the patient is conscious and capable of making decisions about their care.
- Refusal of Treatment or Transport Form: When a patient declines EMS services, this form documents that decision. It includes details on the patient's understanding of the risks involved in refusing treatment or transport.
- Advance Directive or DNR Order: If available, an advance directive or Do Not Resuscitate (DNR) order should accompany the patient care report to ensure that the treatment provided aligns with the patient’s wishes.
- Privacy Notice Acknowledgement Form: This form confirms that a patient has been informed about how their medical information will be used and shared, aligning with HIPAA regulations.
- Insurance Information Form: Collecting the patient’s insurance information is critical for billing purposes. This document should capture details about primary and secondary insurance, including policy numbers and coverage details.
Together with the North Dakota EMS Patient Care Report form, these documents create a complete record that supports effective patient care, ensures legal compliance, and facilitates the accurate billing of services. Ensuring that all appropriate paperwork is completed and properly maintained is essential for the smooth operation of EMS providers and the health care system at large.
Similar forms
The North Dakota EMS Patient Care Report form is similar to hospital admission forms in various aspects. Both documents are designed to capture comprehensive details about the patient's current health condition, medical history, and the treatments administered. Hospital admission forms, like the EMS Patient Care Report, require information on the patient's name, date of birth, social security number, and contact details, ensuring the patient can be accurately identified and billed. They also gather medical information, such as pre-existing conditions, allergies, and medications, which are crucial for providing safe and personalized care. Moreover, both documents have sections dedicated to the care provided during the interaction, including procedures performed, medications given, and the patient's response to treatment. This parallel in content ensures continuity of care from the emergency services to the hospital setting.
Similarly, the form bears resemblance to medical emergency incident reports used by other first responder organizations, such as fire departments and police when they attend to medical emergencies. These reports document the specifics of the incident, including the location, time, nature of the emergency, and any immediate actions taken. Like the North Dakota EMS Patient Care Report, these incident reports detail the patient's condition upon arrival, interventions made, and the outcome of those interventions. Both documents serve a dual purpose: they provide a record of the event and the response for legal, billing, and quality improvement purposes, and they ensure that vital information is communicated to subsequent healthcare providers, which is essential for ongoing patient care.
Another document the North Dakota EMS Patient Care Report is comparable to is the Prehospital Care Report (PCR), commonly used in emergency medical services across the United States. The PCR is a national standard for reporting prehospital medical and trauma care. Both the North Dakota form and the generic PCR collect detailed information about the circumstances of the call, patient demographic information, the medical or trauma assessments performed, interventions initiated, and the patient's response to those interventions. This similarity in structure ensures that irrespective of the location within the United States, EMS professionals are documenting critical patient care information in a systematic and comprehensive manner, facilitating a consistent approach to patient care documentation across the country.
Dos and Don'ts
Completing the North Dakota EMS Patient Care Report form accurately and thoroughly is critical for ensuring the quality of patient care, facilitating billing processes, and maintaining compliance with regulations. The following are recommendations to guide you through filling out the form effectively.
Do:
- Read instructions carefully before beginning, to understand each section's requirements and avoid common mistakes.
- Use black or blue ink for clarity and legibility, ensuring the report is readable for everyone who may rely on the information provided.
- Print legibly in all sections of the form. If your handwriting is difficult to read, consider typing the information if the format allows.
- Include all relevant details in the narrative section to provide a full picture of the patient’s condition and the care provided. This section is vital for subsequent patient care decisions.
- Verify accuracy of medical information, such as pre-existing conditions, medications, and allergies. Double-checking these specifics can prevent medical errors.
- Review the form for completeness before submission. Ensure no sections have been overlooked and all required fields are filled out.
- Use the correct codes and abbreviations approved by your EMS agency and the state of North Dakota. This standardization supports clear communication among healthcare professionals.
- Sign and date the form as required. Your signature attests to the accuracy of the information provided and your adherence to protocols.
- Maintain confidentiality of patient information as per HIPAA regulations. Handle, store, and transmit the form in a manner that protects the patient’s privacy.
Don't:
- Leave sections blank if they are applicable. If a section does not apply, indicate this with “N/A” (not applicable) to demonstrate that the omission was intentional.
- Use correction fluid or tape on the form. Mistakes should be crossed out with a single line, corrected, and initialed to maintain the document's integrity.
- Rush through the form-filling process, which can lead to errors or omissions. Taking your time ensures that the information is as accurate and complete as possible.
- Rely solely on memory for details like medications, medical history, or exact times. Reference available documentation and electronic records whenever possible.
- Include subjective opinions or irrelevant details in the narrative section. Stick to objective observations and pertinent facts related to the patient's care and condition.
- Forget to document patient refusals of service or specific treatments. This information is critical for legal and billing reasons.
- Use ambiguous language that could be interpreted in multiple ways. Be as specific and clear as possible, particularly when describing symptoms, conditions, and actions taken.
- Ignore guidelines for specific fields, such as the correct way to record times (24-hour clock), dates (MM/DD/YYYY), and measurements (use of metric system).
- Discard rough drafts or notes used in completing the form until it is finalized and submitted. These documents can be important if questions arise about the report.
Misconceptions
When it comes to the North Dakota EMS Patient Care Report form, there are several misconceptions that can cloud the understanding of both healthcare professionals and the general public alike. Here, we aim to clarify some of these misunderstandings in an effort to improve comprehension and enhance the quality of emergency medical services.
Misconception 1: The form is only for internal use by EMS personnel. Contrary to this belief, the form serves a dual purpose. It is not only a crucial internal document for EMS teams to record details of the care provided but also a vital piece of communication with other healthcare providers, ensuring continuity of care for the patient.
Misconception 2: Patient consent is not required to fill out the form. In reality, while emergency situations may necessitate immediate care where consent is implied, the form does include sections for the receipt or refusal of service. These sections highlight the importance of patient autonomy and informed consent in the provision of emergency services.
Misconception 3: The form solely focuses on medical interventions. Although medical interventions are a significant component, the form also encompasses a broad range of information including patient demographics, the incident scene's specifics, patient disposition, and even billing information, illustrating a comprehensive approach to patient care.
Misconception 4: All sections of the form must be completed for every call. The form is designed to be as thorough as possible to cover a wide array of situations. However, some sections may not apply to every case. EMS personnel are trained to fill out the form accurately, providing pertinent information relevant to each specific call.
Misconception 5: The narrative section is optional. On the contrary, the narrative section is crucial as it provides a place for EMS personnel to add context and details about the call, patient care, and any deviations from standard protocols, which may not be captured by the form’s structured fields.
Misconception 6: Healthcare providers outside of EMS do not have access to this information. This form often becomes a part of the patient's medical record, accessible to healthcare providers involved in their care post-EMS interaction. It provides a detailed account of the pre-hospital interventions and observations critical for subsequent care decisions.
Misconception 7: Only the physical copy of the form is valid. In the digital age, electronic versions of the EMS Patient Care Report are widely used and accepted. They ensure accurate, legible, and timely documentation that can be easily shared and accessed by various healthcare providers.
Misconception 8: The form is only relevant at the time of the incident. This document has enduring relevance, not only as a record of care provided but also for legal, quality improvement, and educational purposes. Analyzing these reports can lead to enhancements in EMS protocols, training, and ultimately, patient care outcomes.
Understanding the North Dakota EMS Patient Care Report form in its entirety is crucial for effective communication among EMS and other healthcare personnel, ensuring high-quality and coordinated patient care. Clarifying these misconceptions is a step toward demystifying an essential component of emergency medical services.
Key takeaways
Filling out the North Dakota EMS Patient Care Report form accurately and comprehensively is crucial for several reasons. It not only ensures that the patient receives appropriate follow-up care but also supports billing processes and legal documentation. Here are five key takeaways to assist you in the process:
- Complete Patient Information Thoroughly: Include all patient details such as name, date of birth, social security number, and contact information. Accurate identification is essential for patient records and insurance claims.
- Document Incident and Care Details Precisely: Record all incident-related information, including the date, time, location (with GPS coordinates), and the nature of the incident. Detailed documentation of the care provided, including procedures performed, medications administered, and the patient's response to treatment, is critical for both patient care continuity and legal protection.
- Record Mileage and Transport Information: Accurately logging the mileage from the scene to the destination, as well as times related to the dispatch, departure, and arrival, is vital for billing and reimbursement purposes.
- Insurance Information is Key for Billing: Fill in all applicable insurance information, including primary and secondary insurance numbers. Clearly indicate if the patient has no insurance, which affects how billing and payments will be handled.
- Attention to Signatures: Ensure that all necessary signatures, including that of the patient (or responsible party) for service receipt or refusal of service, are obtained. This is crucial for compliance with legal and operational protocols.
Proper completion of the North Dakota EMS Patient Care Report form is not just about fulfilling a requirement; it's about ensuring a continuum of care, facilitating appropriate billing, and adhering to legal standards. Being thorough and attentive to detail can significantly impact the quality of care and operational efficiency.
Browse Popular Documents
North Dakota Charitable Registration - The annual submission of SFN 11302 by charities aids in creating a detailed public record of charitable activities statewide.
Sfn2023 - A $75 fee applies when adding the STEM endorsement between license renewal periods, as stated in the form.
Sfn 847 - The SFN 847 is an essential tool in the administrative process of vehicle sales, making it a vital form for both buyers and sellers.