Printable Sfn 12012 Template
Embarking on any construction or renovation project in North Dakota that exceeds the cost, value, or price of $2,000.00 mandates securing a North Dakota Contractors License as per the instructions on the SFN 12012 form, a crucial detail for every contractor aiming to operate within the legal framework of the state. The license application process, outlined by the Secretary of State, has been methodically structured to ensure compliance with the North Dakota Century Code, Chapter 43-07-07, which further delineates the class and corresponding fee structure for contractor licenses based on job size. From sole proprietorships to corporations, and partnerships in various forms, the form accommodates a range of business entities, each subject to identify their operational structure and provide extensive business and personal identification details. Moreover, the necessity of a North Dakota Sales and Use Tax permit, alongside mandatory workers' compensation coverage verification, underscores the comprehensive nature of the procedural requirements. With provisions for disclosing prior legal complications, bankruptcy involvements, or any history of criminal charges, the form also serves as a declaration of the applicant's legal and financial history. Significantly, non-resident contractors are bound by additional stipulations, agreeing, by virtue of their application, to appoint the Secretary of State as their lawful agent for service of process. All these facets emphasize the SFN 12012 form's role not just as a bureaucratic necessity but as a foundational step towards establishing a legitimate, transparent, and accountable contractor business in North Dakota.
Form Preview
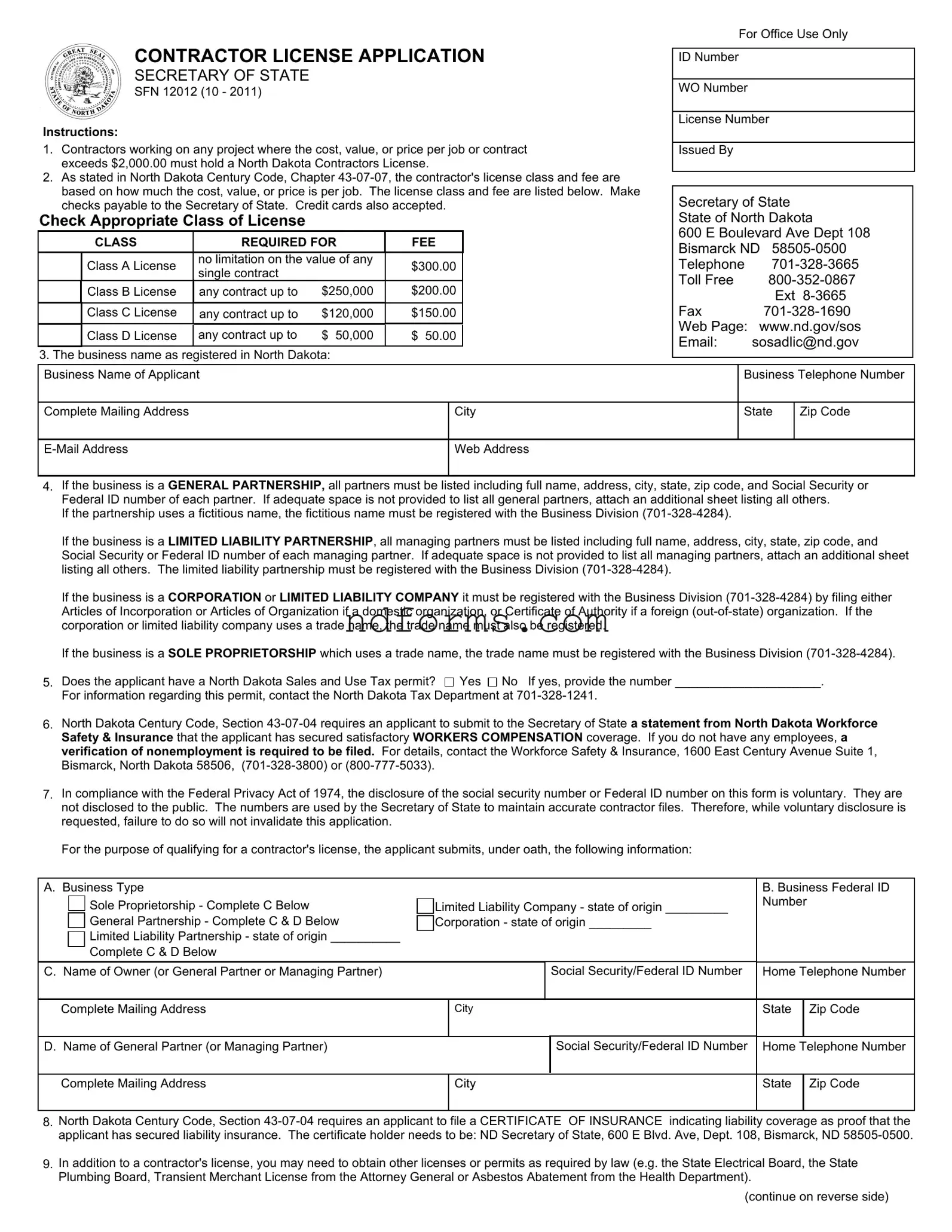
CONTRACTOR LICENSE APPLICATION
SECRETARY OF STATE
SFN 12012 (10 - 2011)
Instructions:
1.Contractors working on any project where the cost, value, or price per job or contract exceeds $2,000.00 must hold a North Dakota Contractors License.
2.As stated in North Dakota Century Code, Chapter
Check Appropriate Class of License
|
CLASS |
REQUIRED FOR |
FEE |
|||
|
Class A License |
no limitation on the value of any |
$ |
300.00 |
||
|
single contract |
|
|
|||
|
|
|
|
|
|
|
|
Class B License |
any contract up to |
$ |
250,000 |
$ |
200.00 |
|
|
|
|
|
|
|
|
Class C License |
any contract up to |
$ |
120,000 |
$ |
150.00 |
|
|
|
|
|
|
|
|
Class D License |
any contract up to |
$ |
50,000 |
$ |
50.00 |
|
|
|
|
|
|
|
3. The business name as registered in North Dakota:
For Office Use Only
ID Number
WO Number
License Number
Issued By
Secretary of State
State of North Dakota
600 E Boulevard Ave Dept 108
Bismarck ND
Telephone |
|
Toll Free |
|
|
Ext |
Fax |
|
Web Page: |
www.nd.gov/sos |
Email: |
sosadlic@nd.gov |
Business Name of Applicant |
|
Business Telephone Number |
|
|
|
|
|
Complete Mailing Address |
City |
State |
Zip Code |
|
|
|
|
Web Address |
|
|
|
|
|
|
|
4.If the business is a GENERAL PARTNERSHIP, all partners must be listed including full name, address, city, state, zip code, and Social Security or Federal ID number of each partner. If adequate space is not provided to list all general partners, attach an additional sheet listing all others.
If the partnership uses a fictitious name, the fictitious name must be registered with the Business Division
If the business is a LIMITED LIABILITY PARTNERSHIP, all managing partners must be listed including full name, address, city, state, zip code, and Social Security or Federal ID number of each managing partner. If adequate space is not provided to list all managing partners, attach an additional sheet listing all others. The limited liability partnership must be registered with the Business Division
If the business is a CORPORATION or LIMITED LIABILITY COMPANY it must be registered with the Business Division
If the business is a SOLE PROPRIETORSHIP which uses a trade name, the trade name must be registered with the Business Division
5. Does the applicant have a North Dakota Sales and Use Tax permit? |
Yes No If yes, provide the number _____________________. |
For information regarding this permit, contact the North Dakota Tax Department at
6.North Dakota Century Code, Section
7.In compliance with the Federal Privacy Act of 1974, the disclosure of the social security number or Federal ID number on this form is voluntary. They are not disclosed to the public. The numbers are used by the Secretary of State to maintain accurate contractor files. Therefore, while voluntary disclosure is requested, failure to do so will not invalidate this application.
For the purpose of qualifying for a contractor's license, the applicant submits, under oath, the following information:
A. Business Type |
|
|
|
|
B. Business Federal ID |
||
Sole Proprietorship - Complete C Below |
Limited Liability Company - state of origin _________ |
Number |
|
||||
|
|
|
|||||
General Partnership - Complete C & D Below |
Corporation - state of origin _________ |
|
|
|
|||
Limited Liability Partnership - state of origin __________ |
|
|
|
|
|
|
|
Complete C & D Below |
|
|
|
|
|
|
|
C. Name of Owner (or General Partner or Managing Partner) |
|
|
|
Social Security/Federal ID Number |
Home Telephone Number |
||
|
|
|
|
|
|
|
|
Complete Mailing Address |
|
City |
State |
|
Zip Code |
||
|
|
|
|
|
|
|
|
D. Name of General Partner (or Managing Partner) |
|
|
|
Social Security/Federal ID Number |
Home Telephone Number |
||
|
|
|
|
|
|
|
|
Complete Mailing Address |
|
City |
State |
|
Zip Code |
||
|
|
|
|
|
|
|
|
8.North Dakota Century Code, Section
9.In addition to a contractor's license, you may need to obtain other licenses or permits as required by law (e.g. the State Electrical Board, the State Plumbing Board, Transient Merchant License from the Attorney General or Asbestos Abatement from the Health Department).
(continue on reverse side)
SFN 12012 (10 - 2011) Page 2
10. Do you hold a contractor license in another state?

 No
No

 Yes If Yes, indicate the state(s)______________________________________________________________________________________
Yes If Yes, indicate the state(s)______________________________________________________________________________________
11.The applicant's experience and/or qualifications to act in the capacity of a contractor. This may include, but is not limited to, the number of years in the business, licenses in other states, detailed explaination of what type of work is being done, training, school, and any other pertinent information.
12. If your answer is "YES" to any of the following questions, give the details on a separate sheet and attach to this application.
a. Has any license been denied, suspended or revoked For you?
For any officer?
For any partner?
For any entity with which you, officers or partners have or are associated with?
Yes

 Yes
Yes
Yes
Yes
No No
No No
b.Have there been any civil lawsuits or arbitration proceedings in which you (or a corporation, limited liability company, or partnership of which you are or were an officer or partner) were involved as a defendant in which fraud or misrepresentation was charged during the
past year? |
As a Defendant |
Yes |
No |
Yes
No
c.Have you or a corporation, limited liability company, or partnership of which you are or were an officer or partner, been involved in bankruptcy proceedings during the past five years?
Yes
No
d.Are there any judgments, arbitration awards, mechanics liens or federal or state tax liens against you, or a corporation, limited liability company, or partnership of which you are an officer or partner, in North Dakota or elsewhere?
Yes |
No |
e. Has the applicant, or officers or partners of the applicant been charged with or convicted of a felony or misdemeanor within the last five years?
Yes
No If Yes, indicate the date, name of the individual charged or convicted, city, state, disposition, and whether a felony or misdemeanor. (This includes ALL crimes, including nonsufficient funds checks, no account checks, and DUIs.)
13.Once the licensing process has started and the requirements are not completed or perfected within 90 days, one half of the filing fee submitted will be retained and the other half returned to the applicant.
14.North Dakota Century Code, Section
AFFIDAVIT
(Sign before a notary)
The Applicant, who is 18 years of age or older, whose name is ________________________________________________________________, being first
duly sworn on oath deposes and says he/she is the applicant above named, or the ______________________________________ of the corporation or a
member of the firm, association, or
this affidavit for and on behalf of said applicant; that he/she has read the within and foregoing application and knows the contents thereof, and that the
statements therein contained are true of his/her own personal knowledge, except as to such statement therein made upon information and belief, and as to
such statements he/she believes the same to be true.
State of ______________________ |
Signature of Applicant |
County of ____________________ |
|
The foregoing instrument was acknowledged before me this ________ day of _______________________, 20 _______.
(Notary Seal/Stamp) |
Notary Public |
|
My Commission Expires______________________________ |
File Attributes
| Fact Name | Description |
|---|---|
| Application Requirement | Contractors must apply for a license using the SFN 12012 form if the cost, value, or price of any project exceeds $2,000.00. |
| License Class and Fee | The class of the contractor's license and the corresponding fee are determined based on the project's cost, with options ranging from Class A (no limit, $300) to Class D (up to $50,000, $50). |
| Governing Law | The requirements for the contractor's license, as outlined in the SFN 12012 form, are governed by the North Dakota Century Code, Chapter 43-07-07. |
| Workers' Compensation Verification | Applicants must provide a statement from North Dakota Workforce Safety & Insurance verifying satisfactory workers' compensation coverage, as required by North Dakota Century Code, Section 43-07-04. |
| Agent for Service of Process | Non-resident applicants must appoint the Secretary of State as their agent to receive legal documents, in accordance with North Dakota Century Code, Section 43-07-19. |
How to Write Sfn 12012
Filling out the SFN 12012 form is a straightforward process that requires attention to detail. Individuals or entities aiming to engage in contracting projects valued over $2,000 in North Dakota must complete this application to obtain the necessary contractor's license. This document plays a crucial role in ensuring that contractors adhere to regulatory standards and possess the requisite credentials to undertake substantial projects within the state.
- Verify the necessity of obtaining a North Dakota Contractors License based on the cost, value, or price per job, which should exceed $2,000.
- Choose the appropriate class of license required for your contracting work. The options include Class A, B, C, or D, depending on the contract's value, with fees of $300, $200, $150, and $50 respectively.
- Provide the registered business name in North Dakota, including the complete mailing address, business telephone number, email address, and web address.
- If your business is structured as a partnership (general or limited liability), list all partners with their addresses, contact information, and Social Security or Federal ID numbers. Attach additional sheets if space is insufficient.
- For corporations or limited liability companies, ensure registration with the Business Division by filing the appropriate documents. If using a trade name, it must be registered as well.
- Indicate whether the applicant possesses a North Dakota Sales and Use Tax permit, providing the permit number if applicable.
- Submit a statement from North Dakota Workforce Safety & Insurance verifying workers' compensation coverage, or a verification of nonemployment, based on your situation.
- Disclose the social security number or Federal ID number as requested, with the understanding that non-disclosure will not invalidate the application.
- File a certificate of insurance indicating liability coverage as proof of secured insurance.
- Check for the necessity of additional licenses or permits as required by law for your specific contracting activities.
- State if holding a contractor license in another state, specifying which state(s).
- Detail the applicant’s qualifications and experience relevant to the capacity of a contractor including years in business, other state licenses, type of work performed, training, and education.
- Respond to mandatory disclosure questions concerning license denial, suspension, or revocation; involvement in litigation; bankruptcy proceedings; judgments or liens; and charges or convictions of felonies or misdemeanors within the last five years, attaching details separately if applicable.
- Acknowledge that incomplete licensing requirements within 90 days will result in the retention of half the filing fee and refund of the remainder.
- Non-resident applicants must sign and file an application appointing the Secretary of State as their true and lawful agent for service of process.
- Complete the affidavit section of the application in the presence of a notary, including the applicant's signature, state, and county of acknowledgment, and the date.
Upon completing these steps and submitting the SFN 12012 form along with the appropriate fees and any required documentation, the application will undergo a review process by the Secretary of State's office. Successful applicants will receive their contractor's license, enabling them to legally undertake contracting projects within North Dakota. It's imperative to maintain compliance with all state regulations and to renew the license as required to ensure ongoing eligibility for contracting work.
Your Questions, Answered
What projects require a North Dakota Contractor's License according to the SFN 12012 form?
Any contractor working on a project where the cost, value, or price per job or contract exceeds $2,000.00 must hold a North Dakota Contractor's License. This requirement ensures that all contractors meet the state's standards for performing construction work.
How are the contractor license classes and fees determined?
The contractor's license class and corresponding fee depend on the project's cost, value, or price. There are four classes:
- Class A License - No limitation on the value of any single contract, with a fee of $300.00.
- Class B License - Contracts up to $250,000, with a fee of $200.00.
- Class C License - Contracts up to $120,000, with a fee of $150.00.
- Class D License - Contracts up to $50,000, with a fee of $50.00.
What information is needed for partnerships applying for a license?
If the business is a general partnership, all partners must be listed with full names, addresses, social security, or federal ID numbers. If it's a limited liability partnership (LLP), all managing partners' details are required. Any additional partners or managing partners beyond the form's space must be listed on an attached sheet. Partnerships using a fictitious name need to register it with the Business Division.
Is a North Dakota Sales and Use Tax permit required for applying?
Applicants must indicate whether they have a North Dakota Sales and Use Tax Permit. If so, the permit number should be provided. Information on how to obtain this permit is available from the North Dakota Tax Department.
What are the insurance requirements mentioned in the SFN 12012 form?
Applicants must submit a Certificate of Insurance showing they have secured liability coverage. The certificate holder must be the ND Secretary of State. This requirement ensures that the contractor has proper insurance to cover any work-related incidents.
What happens if the requirements are not completed within 90 days?
If the licensing process is not completed or requirements are not perfected within 90 days from submitting the application, half of the filing fee will be retained by the office, and the other half will be returned to the applicant. This policy encourages timely completion of the application process.
Common mistakes
Filling out the SFN 12012 form, also known as the Contractor License Application for the state of North Dakota, can be a straightforward process if done carefully. However, applicants often make mistakes due to oversight or misunderstanding, leading to possible delays in approval. Here are four common errors:
- Incorrect License Classification Selection: One frequent oversight is selecting the wrong class of license. The SFN 12012 form outlines different classes based on the contract's cost, value, or price. An incorrect choice could lead to administrative complications or even the rejection of the application.
- Failure to Provide Complete Partner Details: If the business is a partnership, all partners must be listed with their full details. Sometimes, applicants forget to include every partner, especially if there are many, or they submit incomplete information. This omission can slow down the process, as the state needs complete data to proceed.
- Omitting Worker's Compensation and Liability Insurance Documentation: North Dakota law requires applicants to submit evidence of workers’ compensation coverage and liability insurance. Failing to attach these certificates or providing inadequate documentation might result in application delays or denials, as these are critical for safeguarding workers and the public.
- Inaccurate or Incomplete Disclosures: The application asks specific questions about past legal issues, such as license denials, civil lawsuits, and bankruptcy proceedings. Applicants sometimes either inadvertently skip these questions or do not furnish all the required details. Accuracy and completeness in disclosure are vital for regulatory compliance and to avoid potential legal complications.
To mitigate these mistakes, applicants should review the form multiple times, ensure all documentation is prepared and double-checked, and consult the instructions or a legal advisor if there's any uncertainty. Timely and accurate application submission facilitates a smoother licensure process.
- Understanding the scope and limitations of each license class before selection is crucial.
- Maintaining a checklist of required documents, including partnership details and insurance certificates, can be helpful.
- Being open and thorough about past legal or financial troubles by attaching detailed explanations can prevent misunderstandings.
Adhering to guidelines and being meticulous in completing the SFN 12012 form not only demonstrates professionalism but also underscores the contractor's commitment to legal and regulatory compliance in North Dakota. This diligence can lead to a smoother application process and a more robust foundation for business operations.
Documents used along the form
When completing and submitting the Contractor License Application (SFN 12012) form in North Dakota, applicants might need to gather additional documents to ensure a thorough and compliant application process. The following list describes other key forms and documents commonly used alongside the SFN 12012 form. Each of these documents plays a critical role in verifying the eligibility and qualifications of a contractor in North Dakota.
- Certificate of Insurance: This document proves that the applicant has the required liability insurance coverage. The Secretary of State's office needs to be listed as the certificate holder, as indicated in section 8 of the SFN 12012 form. It shows the state that the contractor can cover liabilities for accidents or damages that may occur during a project.
- North Dakota Sales and Use Tax Permit: If an applicant checks “Yes” on the SFN 12012 form indicating they have this permit, they must provide the permit number. This document confirms that the contractor is registered to collect sales tax on the goods and services they provide in North Dakota.
- Statement from North Dakota Workforce Safety & Insurance (WSI): Required by North Dakota Century Code, Section 43-07-04, this statement verifies the contractor’s compliance with state workers' compensation laws, ensuring that they have secured satisfactory coverage for their employees. If the contractor doesn't have employees, they must file a verification of nonemployment.
- Proof of Business Registration: Depending on the business structure (e.g., GENERAL PARTNERSHIP, CORPORATION, LIMITED LIABILITY COMPANY), the appropriate registration documents with the North Dakota Secretary of State’s office are necessary. This could include Articles of Incorporation, Articles of Organization, or a Certificate of Authority for foreign entities.
Together, these documents complement the SFN 12012 form, providing a comprehensive overview of the contractor's legal, operational, and financial standing. Collecting and submitting these documents as required supports a smooth and effective application process for a North Dakota Contractor’s License.
Similar forms
The SFN 12012 form, designated for contractor license applications in North Dakota, bears similarities to various other documents pertinent to business operations and regulatory compliance. Each document shares features with the SFN 12012 form, such as the purpose of ensuring businesses meet state-imposed requirements before operating within a jurisdiction.
Business Registration Forms are similar to the SFN 12012 form in that they require basic information about the business entity, including its name, address, and type of business structure. Like the SFN 12012, which necessitates details on the business type and its partners or owners, business registration forms serve as a preliminary step to formalize a business’s presence under state law. These forms, which may be filed with a state's business registry or Secretary of State, share the goal of establishing a legal framework for operations, liability, and taxation purposes.
Professional License Applications also parallel the SFN 12012 form regarding their role in ensuring individuals or entities meet specific professional standards before offering services to the public. These applications often require proof of qualifications, such as education, training, and previous licensure, similar to how the SFN 12012 form requests details on the applicant’s experience and qualifications in the contracting field. The key similarity lies in their purpose to protect the public by ensuring only qualified practitioners are licensed to operate.
Permit Applications for Specific Projects, required for particular types of construction or business projects, share a commonality with the SFN 12012 form in terms of regulating activities that impact public safety and welfare. These permits might demand detailed plans of the proposed work, similar to how the SFN 12012 requires information on the contractor’s ability to perform the job, including prior experience and relevant qualifications. The focus on safety, compliance, and accountability underscores their similarity.
Zoning and Land Use Applications are another category of documents akin to the SFN 12012 form. While zoning applications specifically deal with the use of land and adherence to local ordinances, they require applicants to submit detailed plans and justifications for their projects — a process not unlike the specificity required in the SFN 12012 form concerning the scope of work and expertise of the contractor. These documents collectively ensure that business operations and physical projects align with community standards and legal requirements.
Overall, the SFN 12012 contractor license application form shares multiple similarities with other regulatory and compliance documents, emphasizing the importance of thorough vetting in business and professional practices to uphold public safety, legal standards, and industry integrity.
Dos and Don'ts
When filling out the SFN 12012 form for a contractor license application in North Dakota, there are important dos and don'ts to keep in mind. This guidance aims to help applicants navigate the process with ease and ensure that their application stands the best chance of being processed without unnecessary delays.
- Do ensure you meet the requirement of needing a contractor's license for projects exceeding $2,000.00 in cost, value, or price per job as specified.
- Do select the correct class of license based on the cost, value, or price of your jobs, ensuring the fee you pay matches the class required.
- Do provide accurate and complete information for your business name as registered in North Dakota, including full details required in the form for the type of business entity you're registering.
- Do list all required partners or members if your business is a partnership or limited liability partnership, using additional sheets if the space provided isn't sufficient.
- Do include your North Dakota Sales and Use Tax permit number if you have one, as it's necessary for completing your application.
- Don't forget to submit a statement from North Dakota Workforce Safety & Insurance to demonstrate that you have secured satisfactory workers' compensation coverage, or verification of nonemployment if applicable.
- Don't overlook the requirement to file a Certificate of Insurance indicating liability coverage, making sure the certificate holder is the ND Secretary of State as specified.
- Don't ignore questions related to previous license denials, suspensions, or revocations, lawsuits, bankruptcies, liens, and criminal charges. Transparency is key, and additional sheets should be attached if you answer "YES" to any of these queries.
Remember, the accuracy and completeness of your application are critical. This not only includes providing all necessary information but also ensuring that you understand the commitments and responsibilities involved. A clear and correctly filled application form serves as the first step toward obtaining your contractor's license in North Dakota.
Misconceptions
When it comes to understanding the SFN 12012 form for contractor license applications in North Dakota, there are several misconceptions that can complicate the process for applicants. Below are six common misunderstandings and clarifications that aim to shed light on these areas.
- Misconception #1: The SFN 12012 is only necessary for large-scale contractors.
In reality, this form is required for any contractor working on a project where the cost, value, or price per job exceeds $2,000.00. This applies not only to large-scale operations but also to smaller contractors and independent professionals. - Misconception #2: Filling out the form is all that's required to obtain a license.
Completing the SFN 12012 form is just the first step. Applicants also need to submit additional documentation, such as proof of liability insurance and workers' compensation coverage, and may need to comply with further state or local requirements. - Misconception #3: The license class and fee structure is based on the contractor's experience.
The license class and corresponding fee are determined by the monetary value of the contract or job, not the contractor's level of experience or years in the business. - Misconception #4: Once submitted, the application process is quick and requires no further action.
The process can be lengthy and may require additional steps or documentation. If the licensing requirements are not completed or perfected within 90 days, only half of the filing fee is refunded, emphasizing the need for timely and accurate completion of all application requirements. - Misconception #5: Sole proprietors do not need to declare a trade name on the SFN 12012 form.
If a sole proprietorship operates under a trade name, that name must be registered and declared in the application process. This requirement ensures that all business entities are properly registered under their operating names. - Misconception #6: Social Security or Federal ID numbers are optional in the application.
While the disclosure of these numbers is stated as voluntary, not providing them can complicate the process. These numbers are used by the Secretary of State to maintain accurate contractor files and facilitate the application process.
Understanding these misconceptions can streamline the application process for the SFN 12012 form, helping contractors ensure compliance with state requirements and aiding in the successful acquisition of a contractor's license in North Dakota.
Key takeaways
Understanding the SFN 12012 form is crucial for contractors planning to undertake projects in North Dakota. Here are key takeaways about filling out and using this form:
- Contractors aiming to work on projects with costs exceeding $2,000.00 must hold a valid North Dakota Contractors License, as mandated by the state.
- The license class and accompanying fee depend on the project's cost, with four distinct classes (A, B, C, and D) catering to different project sizes and financial ceilings.
- It's necessary for applicants to provide the business name registered in North Dakota along with a complete mailing address, telephone number, and email if applicable.
- Depending on the business structure (General Partnership, Limited Liability Partnership, Corporation, or Sole Proprietorship with a trade name), specific details about partners or managing members must be included. Additional sheets may be attached if the space provided is insufficient.
- An active North Dakota Sales and Use Tax permit number is required, highlighting the legal obligation to comply with state tax regulations.
- Applicants must also submit a statement from North Dakota Workforce Safety & Insurance confirming satisfactory Workers' Compensation coverage, or a verification of nonemployment if there are no employees.
- Providing a Social Security or Federal ID number on the form is voluntary but essential for maintaining accurate contractor files, in accordance with the Federal Privacy Act of 1974.
- A Certificate of Insurance must be filed with the application, proving that the applicant has secured liability insurance adequate for conducting business in the state.
- The form also inquires about additional licenses or permits, previous contractor licenses in other states, and any relevant legal or financial issues that might affect the applicant’s eligibility.
This comprehensive approach ensures that all contractors operating in North Dakota meet the regulatory and safety standards necessary for the state’s construction industry.
Browse Popular Documents
51/50 Law - Serves as a guide for navigating the legal requirements and procedural steps for seeking intervention for someone unable to voluntarily seek help due to their mental state.
Sfn Conference 2023 - The capacity to attach addendums allows for the inclusion of extensive descriptions or additional information beyond the form's initial provisions.
Ems Agencies Near Me - Includes a narrative section for EMS personnel to describe the incident, care provided, and any other relevant observations in detail.